
Vaccination Campaigns and Coverage Prior to 1930
This post is a continuation of my series about the causes of chronic disease epidemic we are currently experiencing in the 21st century. In my previous articles, I have discussed that vaccines are by far the most significant driver of all serious chronic illness, and nearly 100% of it in children. I am currently focusing on cancer, the 2nd leading cause of death in the US after cardiovascular disease:
According to the latest CDC data (2024), the top 3 causes of death in the United States are:
- Heart disease — 683,491 deaths
- Cancer — 619,876 deaths
- Accidents (unintentional injuries) — 197,449 deaths
In my previous post, I dove into the 175+ years of rising rates of cancer per 100K population in the US using extremely high quality data from 1915 Prudential Life Insurance actuarial report (Hoffman report). The report demonstrated that prior to the 19th century, cancer had not been the constant threatening presence of human life as we are lead to believe. In fact it was almost unheard of. However, mysteriously, during 19th century cancer rates rose from near absence to quite significant numbers. Even more mysteriously, it affected primarily “civilized” people, those who had access to the modern scientific medicine. As the Hoffman report demonstrated with actuarial precision, the rise of cancer over the span of the 19th century was a real trend, and NOT due to aging population, improved diagnostics, environmental/occupational exposure to toxic materials, and lack of medical care. It was often inversely correlated with racial differences (the “primitives” did not have cancer) and with socioeconomic differences (the relatively affluent classes had much more of it). The Hoffman report, despite its 800+ page volume, exactness and investigation of numerous possible factors, never mentioned the word “vaccine” even once. To me that looks like a tell – the authors already knew that vaccines were responsible. Numerous contemporaneous accounts of medical doctors confirm this. Doctors who practiced medicine instead of chasing profits via “gold standard science” knew what was killing people and animals – injection of poison from rotting putrid concoctions pushed as “protection”. Here are some illustrations of cancers developed from vaccination sites, late 1800s-early 1900s:

X’s mark the spots of mRNA vaccinations – looks familiar, doesn’t it?

However, for the establishment, of which Prudential was a big part, the rise of cancer was welcome news. The people were being silently poisoned in a very profitable way, and fear of this mysterious devastating illness would sell even more life insurance policies at even greater premiums!
When I write about vaccines being by far the leading cause of cancer (or pick another chronic illness), I frequently get pushback – but there was no vaccines, or practically none back when! I decided to investigate vaccination coverage, major campaigns and related law prior to 1930, focusing on United States and Europe. Both regions had experienced a rapid rise of cancer, with Europe and especially UK being somewhat ahead of the US. Both regions shared population due to mass immigration to the US.
The period from 1798 to 1929 can be characterized as the first generation of human vaccinology. It started with Jenner’s variolation for smallpox (cowpox lymph). You can read about the discovery of the method from Circassians, a tribe that raised girls for sale to Turkish harems, by Lady Montague, the wife of the British Ambassador to Constantinople, in this post. By 1929, several vaccines were already in wide use: live attenuated viral (smallpox, rabies), killed bacterial (cholera, typhoid, plague), biologicals (toxoids) against diphtheria, and a live attenuated mycobacterial product (BCG). What did not exist in 1798 and was only loosely emerging by 1929 was a statistical infrastructure for measuring population coverage. However, civil registration, vital statistics, school attendance records, and military medical reports developed in parallel with the vaccines themselves, and most of the figures reproduced in this post are by-products of those state-building (aka, population surveillance and control) initiatives.
2. Smallpox: the first mass enforced vaccine
Smallpox was a major cause of death in eighteenth-century Europe. The true cause of it remains unknown (no, it’s not a virus), however, the illness is known to be associated with unsanitary living conditions, crowding, polluted water and possibly exposure to chemicals such as arsenic and mercury. Death registries available in Sweden state that smallpox accounted for about 10%-15% of the annual Swedish deaths in the late 1700s[1]. In London, where parish burial registers are well detailed, smallpox accounted for roughly 7 to 10 per cent of all deaths through most of the eighteenth century and produced age-standardized mortality of about 3,000 per million per year, falling to fewer than 100 per million by the closing decades of the nineteenth century[2].
Edward Jenner’s Inquiry into the Causes and Effects of the Variolae Vaccinae was published in 1798, and Jennerian vaccination spread by personal correspondence and demonstration with extraordinary speed. By 1801 vaccination had reached Vienna, Geneva, Hanover, Boston, and the Spanish court; the Spanish Royal Philanthropic Vaccine Expedition (1803–1806), led by Francisco Javier de Balmis, carried lymph in arm-to-arm succession aboard a small frigate to the Canaries, Venezuela, New Granada, New Spain, the Philippines, and Macao. In Britain, the Royal Jennerian Society was founded in 1803 with Jenner as president, dissolved by 1809, and replaced by the state-funded National Vaccine Establishment in 1808[3]. In its founding decade the National Vaccine Establishment was primarily a distribution hub rather than a clinic: in 1810 it recorded only 2,087 vaccinations at its London stations but issued 19,685 charges of vaccine lymph to 3,973 practitioners across the country.
Voluntary uptake nevertheless reached substantial levels in some jurisdictions even before any law required vaccination. In Napoleonic France, where Jenner was personally celebrated and where Napoleon ordered the vaccination of the army in 1805, the share of registered births vaccinated in the first year of life rose to above 50 per cent in 1811 to 1815 and to over 80 per cent in 1816 to 1820[4]. These figures are remarkable (if true): they imply that France achieved roughly the coverage level that England would only get after a generation of compulsion.
The Vaccination Act of 1853 made infant vaccination against smallpox compulsory in England and Wales: every child was to be vaccinated within three months of birth, and parents who refused were liable to a fine of twenty shillings. The 1853 Act was the first national mandatory vaccination law in any major industrial state and the model on which most subsequent European laws were drawn. The 1867 Act tightened enforcement and authorized cumulative penalties; the 1898 Act, after a generation of growing dissent, introduced a conscience clause exempting parents who could persuade a magistrate that they sincerely objected.
The coverage figures generated by these laws are the largest dataset of their kind in the nineteenth century, but they have to be read with care. The official ratio reported by the Registrar-General was ‘public vaccinations as a share of registered births’ in a given year. In the first six years after compulsion (1853 to 1859) the ratios were 62.6, 112.1, 74.5, 67.9, 65.1, and 71.5 per cent respectively[6]. The 1854 figure of 112 per cent reflects an effort to vaccinate older children who had been missed before the Act. Once that lag was worked off, the ratio stabilised around two-thirds of births.
The 1898 conscience clause produced a documented and well-studied reversal. In its first year, English magistrates issued more than 200,000 certificates of exemption; in the years that followed, the annual rate of new exemptions stabilized at roughly 30,000 to 33,000[8]. The geographical distribution of refusal was highly uneven: in Leicester, the center of the English anti-vaccination movement, the share of infants exempted reached 80 to 90 per cent in the early 1900s, while in much of the rest of the country exemption rates remained in single figures[9]. The Leicester case is important because it falsifies the otherwise plausible inference that compulsion necessarily produces high coverage: the city achieved low smallpox mortality through isolation and notification (the ‘Leicester method’), with very little vaccination of infants.
The European smallpox epidemic of 1870–1874 was triggered by the devastation of the Franco-Prussian War[10]. This provided the immediate political occasion for the Reichsimpfgesetz of April 8 1874, which made primary vaccination of every child within their first two years and revaccination at the age of twelve compulsory across the new German Empire[11]. The law remained in force until 1982 in West Germany and 1983 in the GDR.
Similar law for compulsory infant vaccination was enacted in Sweden on March 6, 1816, under King Karl XIII. The law required parents to have their children vaccinated within two years of birth, drew on the parish-register surveillance infrastructure of the Swedish Lutheran church, and made Sweden the first country in continental Europe with a national legal mandate[13].
The United States: state-by-state authority and Jacobson
The first compulsory vaccination law in any jurisdiction was passed by the Commonwealth of Massachusetts in 1809. The American constitutional structure made vaccination a matter of state and municipal authority, with no national mandate. By 1905, when the United States Supreme Court decided Jacobson v. Massachusetts, eleven of the then forty-five states had statutory authority for compulsory vaccination during epidemics, and several additional states had school-entry requirements[15]. The Supreme Court upheld the Cambridge, Massachusetts ordinance by 7 to 2; Jacobson’s fine was five dollars, equivalent to roughly 170 dollars in 2025 currency. No reliable national US coverage figure exists for the nineteenth century: enforcement was patchwork, vital statistics were collected by individual cities, and the federal Public Health Service did not undertake systematic immunization surveillance until the twentieth century[16].
Japan: the Meiji project
Japan’s adoption of European vaccination predates the Meiji Restoration by several decades. Cowpox lymph reached Nagasaki in 1849, and Kanagawa, Edo, Kyoto, and Osaka had vaccination dispensaries by the late 1850s. The Meiji government made vaccination compulsory by ordinance in 1872; it was administered by police-certified vaccinators and verified by certificate checks during outbreaks. Coverage was achieved unevenly across the prefectures: in Fukui Prefecture, for example, vaccination rates only crossed 80 per cent in the second half of the 1880s, more than a decade after the national mandate[17]. The Vaccination Law was revised in 1909 to require revaccination, on the German model.
Colonial India:
Vaccination in British India was the largest single smallpox program in the world in terms of absolute numbers vaccinated, but the smallest as a share of the population it ostensibly covered. The Compulsory Vaccination Act of 1880 applied only to municipalities and cantonments, which together contained a small fraction of India’s roughly 280 million people; rural India remained, in practice, voluntary[18]. Annual vaccinations rose dramatically across the second half of the nineteenth century: in Bengal, the United Provinces, and Punjab combined, vaccinations rose from about 556 in 1864–65 to more than 5 million in 1902–03[19]. Expressed as a share of total population, however, the all-India vaccination rate was 2.7 per cent in 1880–81 rising to 3.5 per cent in 1902–03; expressed as successful primary vaccinations of the birth cohort, the rate moved from 19.9 per cent in 1880–81 to 39.1 per cent in 1902–03. The population coverage that remained below European levels until well after independence.
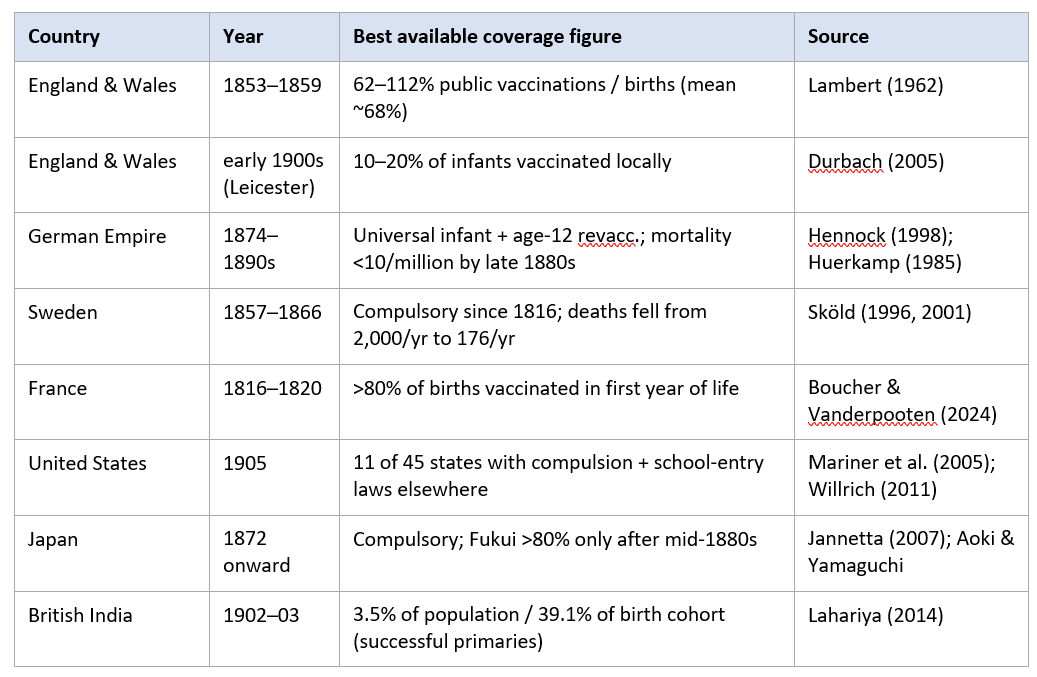
Summary table of smallpox vaccination coverage
3. Rabies: Pasteur and the first “medically supervised” vaccine
On 6 July 1885, Louis Pasteur began a course of thirteen (!!!) subcutaneous injections of “attenuated rabies virus” in the nine-year-old Joseph Meister, who had been bitten fourteen times by a rabid dog two days earlier in the Alsatian village of Maisonsgoutte. Meister reportedly survived[20]. No information about him or his health status subsequent to this experiment is available. The second famous case, Jean-Baptiste Jupille, was begun on 20 October 1885 and Pasteur reported the two cases together to the Académie des Sciences on 26 October. By 1 March 1886, Pasteur was able to report to the Académie that he had treated 350 patients with one death; the published series in the Comptes Rendus of November 1886 reported 2,496 persons inoculated through 31 October 1886, of whom roughly half (1,726) came from France or Algeria and the remainder from twenty-five other countries[21].
Rabies “virus” and vaccines are one of the most tragic scams of all times, which developed an entirely new illness that did not exist prior to Pasteur’s “invention” – paralytic rabies, a direct result of his injections.
Within five years of Meister’s treatment, rabies treatment centers modelled on Pasteur’s protocol had opened on every inhabited continent. The Instituto Pasteur do Rio de Janeiro was inaugurated on 25 February 1888, nine months before the Paris institute itself; the first Brazilian rabies treatment, of Isolina Torres, took place on 9 February 1888[25]. The New York Pasteur Institute opened on 18 February 1890 under Paul Gibier[26]; the Pasteur Institute in Saigon was founded by Albert Calmette in 1891 as the first colonial branch in the French network; Tunis followed in 1893, Algiers in 1894, and Lille was founded in 1894 and inaugurated in 1899. By the CDC’s reckoning, by 1890 there were rabies treatment centers operating in Budapest, Madras, Algiers, Bandung, Florence, São Paulo, Warsaw, Shanghai, Tunis, Chicago, New York, and many other cities[27].
In British India, the Pasteur Institute at Kasauli opened in August 1900 under Major (later Sir) David Semple of the Indian Medical Service; it was the first Pasteur Institute in the British Empire. The Pasteur Institute of Southern India at Coonoor opened on 25 April 1907 and began rabies prophylaxis on 7 April 1907[28]. The two institutions together became the largest rabies treatment centers in the world by the inter-war period. Patient numbers at Coonoor and its franchises rose from fewer than 200 in 1907 to roughly 13,000 in 1935; at Kasauli, 21,898 patients were treated in 1935, of whom 16,627 received the full course, with 86 deaths, a case-fatality of 0.52 per cent[29]. A precise cumulative figure for Paris through 1900 or 1920 has not been published in any open-access secondary source consulted; the relevant series is contained in the Annales de l’Institut Pasteur and the institute’s archived annual reports.
4. Cholera, typhoid, and plague: the bacterial vaccines
The concept of vaccination for an allegedly bacterial illness is even stupider than the concept of vaccination against “viruses”. Bacteria are animals. They are single-cell organisms, but nevertheless, they are whole, complete, independent species. Vaccination against bacteria is therefore just as ridiculous as vaccination against horses, tigers or wolves.
Koch is credited with “culturing” the cholera bacilli in mid 1800’s, which became known as “the comma bacillus”. Koch claimed he isolated the organism from cholera patients and grown it in culture, fulfilling only two of his famous “postulates” for proving causality, but he had yet to fulfil the third, i.e. to show that pure cultures of the comma bacillus obtained from cholera victims could cause the disease in an animal model. This third postulate remained undemonstrated for the next 75 years, as no cholera could be produced directly by using Koch’s claimed causative agent, i.e. “isolated and cultured bacilli”! In 1959 Sambhu Nath De claimed the discovery of the cholera “toxin” i.e. an invisible excretion from bacterium, in Kolkata, India. I reviewed that study and details are available in the post linked above. It is an utter unscientific nonsense and fraud. No causality of cholera by cholera bacterium or its alleged toxin has ever been scientifically established.
Lack of scientific proof of disease causation has never stopped a vaccinator from profit extraction. When you cannot fine a cause, just presume a “virus” or a bacterial “toxin” – both invisible, both produced by the same methods of collecting puss, decaying organs, grinding them up, filtering and when you see nothing, that’s it! You got that “pathogen”. The first human use of a killed (partly attenuated) bacterial vaccine on a population scale was Jaime Ferrán i Clua’s cholera vaccine, deployed during the 1885 Valencia epidemic in eastern Spain. Ferrán’s product was a live attenuated culture of Vibrio cholerae derived from a Marseilles outbreak the previous year. He administered it to more than 30,000 people in Valencia in the spring and summer of 1885; the often-cited 50,000 figure appears to be a popular embellishment and cannot be traced to a primary source[30]. Ferran’s trial design lacked controls and his statistical claims were quickly disputed by the French and German bacteriologists who had hoped to win the Prix Bréant for the first cholera vaccine.
Waldemar Haffkine, a Russian-born bacteriologist working from Pasteur’s laboratory in Paris, developed a heat-killed cholera vaccine in 1892 and carried out the first controlled field trial of any cholera vaccine in the Kattal Bagan slum in Calcutta from March 1894.[31]. By autumn 1895, Haffkine reported to the Indian Medical Service that approximately 42,000 people had been inoculated against cholera in the tea plantations of Bengal, Assam, and Punjab[32]. Waldemar Haffkine (real name Modrecai Chavkin) was a true Odessa extract, a conman who attached himself to Metchnikov and subsequently to Pasteur’s vast government-sponsored empire of zealous vaccinators and rose to quite some lofty science heights. He was also a true believer and jabbed himself a few times with his concoctions. More about his plague adventures below.
Typhoid: Wright, the Boer War, and World War I
I briefly covered the mysterious “typhoid” – an alleged “bad” salmonella toxin, which does not exist in “normal” salmonella. I am quite certain typhoid was an early example of rebranding vaccine injuries (smallpox or another contemporaneous vaccine injury, such as rabies shots). As I have written in this post:
Today typhoid is claimed to be caused by bacterium salmonella, subtype typhi. It is further claimed, quite incredibly, to be a systemic blood infection vs gastrointestinal infection for both cholera and “regular” non-typhi salmonella. I find it incredible that a systemic blood infection, a mass human illness in mid 19th century United States could be caused simply by the “bad drinking water”! How does the typhi agent get INTO the blood stream? Why doesn’t the cholera or non-typhi salmonella “agents” do the same? Cholera is a massive gastrointestinal upset, sometimes so violent to be lethal. Dilation of the intestinal walls in theory can provide access for the products to the blood, yet cholera “agents” seem not as nimble as the typhi “agents”!
Almroth Wright developed his heat-killed typhoid vaccine at the Army Medical School in Netley between 1896 and 1898 and tested it on more than 3,000 British soldiers at military stations in India before the Second Anglo-Boer War[33]. During the Boer War itself (1899–1902), Wright’s vaccine was offered to soldiers on a voluntary basis. Of approximately 448,000 British soldiers dispatched to South Africa, only about 14,000 accepted inoculation; more than 8,000 died of typhoid and roughly 58,000 were hospitalized, “a public scandal that fundamentally reshaped military medical policy” as stated in this source [34]. Except, of course, it reshaped nothing. Experimentation with poison shots on military servicemembers continues to this day.
World War I provided further opportunities for large-scale human experimentation. The British Army produced and issued approximately 10 million doses of typhoid vaccine over the course of the war, and from 1915 more than 90 per cent of troops dispatched overseas received the vaccine of roughly 4.97 million[35].
Plague: Haffkine (Chafkin) in Bombay
The third plague pandemic, which spread from Yunnan via Hong Kong from 1894, reached Bombay in 1896. Haffkine moved from Calcutta to Bombay in October 1896 to develop a vaccine and on 10 January 1897 administered the first dose of his heat-killed Yersinia pestis vaccine to himself, using ten milliliters, four times the planned human dose[37]. The first controlled trial was conducted at the Byculla House of Correction in Bombay in January and February 1897.
Production at the Plague Laboratory at Parel scaled rapidly. By 1900–1901 plague vaccine recipients in India had reached approximately four million, and between 1897 and 1925 an estimated 26 million doses of Haffkine’s anti-plague vaccine were shipped from Bombay across the British Empire[38]. Blaming vax failures on “contaminated vials” was already an established gaslighting method back then. In the so-called “Mulkowal disaster” of 1902, nineteen villagers died of tetanus (!) and their deaths were blamed on a single contaminated bottle (53N) of the plague vaccine. This incident suspended Haffkine’s directorship until his exoneration by the British government in 1907[39]. Please remember this next time you are propagandized about the need to get a tetanus shot. Tetanus does not exist. It is a serious vaccine injury.
The Manchurian plague, 1910 to 1911: a vaccine that did not work
The Manchurian pneumonic plague epidemic of 1910–1911 killed approximately 60,000 people in north-eastern China, with a case-fatality close to 100 per cent. Wu Lien-teh, who led the international response, attempted limited use of conman Haffkine’s bubonic plague vaccine, particularly in the Russian zone under D. K. Zabolotny; the official report of the International Plague Conference held at Mukden in April 1911 concluded that vaccination had played no significant part in controlling the outbreak[40]. No licensed pneumonic plague vaccine exists today.
Another more recent attempt at making a plague vaccine with an illegal human experiment by the US DOD is documented here. It failed, too.
5. Diphtheria and BCG
Diphtheria antitoxin, developed independently by Emil von Behring and Émile Roux in 1890 to 1894, is not strictly speaking a vaccine: it confers passive immunity through injection of horse-derived antibodies. It belongs in this report because its administration anticipated, and partly trained the institutional muscle for, the mass immunization campaigns that followed. Roux reported to the 1894 International Hygiene Congress in Budapest that case-fatality among children with diphtheria treated with serum at the Hôpital des Enfants-Malades in Paris had fallen from about 50.7 per cent to about 24.5 per cent[41]. Hermann Biggs and William H. Park introduced antitoxin production at the New York City Department of Health in late 1894; by 1895 the Department was maintaining a stable of approximately sixty horses and produced more than 25,000 protective doses in its first year[42]. New York City diphtheria deaths fell from 2,870 in 1894 to about 1,400 in 1900, a 51 per cent reduction over six years, in a city whose population was growing rapidly[43].
Béla Schick devised in 1913 the skin test that bears his name, allowing prospective identification of children susceptible to diphtheria. From 1921, William H. Park and Abraham Zingher at the New York City Department of Health began a systematic Schick-test-and-vaccinate campaign in the city’s public and parochial schools, using a toxin-antitoxin (TAT) mixture as the immunizing agent. Park and Zingher reported in 1923 that more than 150,000 children had been Schick-tested in the boroughs of Manhattan and the Bronx; in the cohort followed across the winter of 1921–22 they recorded only 14 cases of diphtheria among the vaccinated children compared with 56 in an equal-size unvaccinated cohort[44]. By 1927 Park’s series reached roughly 90,000 vaccinated and 90,000 unvaccinated matched children, with a fourfold lower diphtheria attack rate in the vaccinated group.
Outside New York, the largest pre-1930 diphtheria immunization campaign was conducted by Connaught Laboratories in Toronto using the diphtheria toxoid that Gaston Ramon had developed at the Pasteur Institute in 1923. Between September 1925 and February 1927 the Connaught field trial covered approximately 120,000 children in nine Canadian provinces; the Toronto city program of December 1926 to June 1929 vaccinated 36,000 children directly, and reduced diphtheria incidence in the Toronto–Hamilton region by approximately 90 per cent in the following decade[45]. Canada reported approximately 9,000 cases of diphtheria nationally in 1924; by the mid-1930s the figure had fallen to a few thousand. Routine diphtheria immunization only became compulsory in France in June 1938, fifteen years after Ramon’s discovery, so French coverage figures before 1930 are modest and were not located in a verifiable form for this report.
The Bacille Calmette–Guérin (BCG) vaccine against tuberculosis was the product of thirteen years of passage of Mycobacterium bovis on bile-potato medium at the Pasteur Institute in Lille and Paris from 1908. The first human dose was administered orally by Benjamin Weill-Hallé, assisted by Raymond Turpin, to a newborn at the Hôpital de la Charité in Paris on 18 July 1921[46]. The vaccine was given orally to neonates and only later, in the 1940s, became a routine intradermal injection. In a report published in the Annales de l’Institut Pasteur in 1927, Calmette and colleagues reported the first 21,200 vaccinations; by 1928 the cumulative figure was approximately 114,000 infants vaccinated, principally in France but also in French colonies including Madagascar and Indochina[47]. The Health Committee of the League of Nations endorsed BCG safety in 1928, and the strain was shared with Soviet bacteriologist Lev Tarasevich in 1925, with the first Soviet vaccinations of neonates in TB-endemic regions reported in 1928[48]. Linda Bryder’s comparative study of BCG adoption in Scandinavia, Britain and the United States traces an unusually cautious uptake in the Anglophone world that continued into the post-war period; Olaf Heimbeck’s 1927 trial of BCG in student nurses at Ullevål Hospital in Oslo, with strikingly favourable results, was the principal Scandinavian point of entry[49].
Another “bad batch” – the Lübeck disaster, 1929–1930
Between December 1929 and April 1930, 251 newborns at the Lübeck municipal hospital in northern Germany were given three oral doses of BCG that had been contaminated, in the hospital’s own laboratory, with a virulent Mycobacterium tuberculosis culture used for diagnostic purposes. Seventy-two of the infants died of tuberculosis; 173 survived with radiologically or clinically detectable infection; only a handful escaped infection. The episode is the largest documented vaccine-safety catastrophe before the Cutter incident of 1955[50]. The hospital director, Ernst Altstaedt, was sentenced in 1932 to 15 months’ imprisonment for negligent homicide.
The vaccinators learned from those early mistakes. That’s why we have the NVIC law and the PREP Act today. By accepting vaccinations you automatically waive all constitutional rights, all natural law rights and any rights as a human being whatsoever. You simply cannot sue for death of injury from these idiotic things. Please learn already!
https://sashalatypova.substack.com/p/vaccination-campaigns-and-coverage